Stoicism and Personality Disorders: Sage vs. Anti-Sage
Table of Contents
- Introduction
- Understanding Stoicism
- The Stoic Sage vs. the Anti-Sage
- Narcissistic and Borderline Personality Disorders
- Moral Responsibility and Personality Disorders
- Irrational Thoughts and Negative Emotions
- Splitting and Object Relations Theory
- Comparative Analysis of Moral Values
- Therapeutic Approaches: From Moral Treatment to Healing
- Societal and Moral Implications

Chapter 1: Introduction
“The happiness of your life depends upon the quality of your thoughts: therefore, guard accordingly, and take care that you entertain no notions unsuitable to virtue and reasonable nature.”¹
The quest to comprehend human behavior, particularly the moral dimensions that govern our actions, has been a central theme in both philosophy and psychology throughout history. Stoicism, an ancient Greek philosophy, asserts that our perceptions and judgments are the true sources of our emotional well-being or distress. As Epictetus succinctly stated,
“Men are disturbed not by things, but by the views they take of them.”²
This perspective emphasizes the profound power of rational thought and virtue in achieving a tranquil life.
In contrast, modern psychology identifies certain personality disorders — specifically Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD) — where individuals exhibit patterns of irrational thinking, emotional instability, and morally questionable behaviors.³ These disorders challenge societal norms and raise critical questions about moral responsibility and the capacity for personal change.
This comparative analysis seeks to bridge the timeless insights of Stoic philosophy with contemporary understandings of NPD and BPD. By examining the moral values espoused by Stoicism alongside the moral implications inherent in these personality disorders, we aim to demonstrate the validity of the Stoic assertion that it is not external events that disturb us, but our interpretations of them. This idea resonates with Albert Ellis’s Rational Emotive Behavior Therapy (REBT), which posits that irrational beliefs are the root cause of emotional distress.⁴
We will explore the concept of the Stoic sage — a person who has achieved moral and intellectual excellence — and contrast it with what could be termed the “Anti-Sage,” exemplified by individuals exhibiting traits characteristic of NPD and BPD. We will learn how these disorders manifest as moral conditions, necessitating not only clinical intervention but also moral guidance and transformation.⁵
Furthermore, we will investigate the role of defense mechanisms such as “splitting,” as understood in Object Relations Theory, in perpetuating the dysfunctional patterns observed in NPD and BPD.⁶ By understanding these mechanisms, we can appreciate the challenges individuals face in integrating positive and negative perceptions of themselves and others — a crucial obstacle in their moral and emotional development.
Through this exploration, the paper will address several critical questions:
- How do Stoic principles explain the emotional turmoil experienced by individuals with NPD and BPD?
- In what ways are NPD and BPD moral conditions, and what are the implications for treatment and moral responsibility?
- How can therapies that incorporate moral guidance, such as Dialectical Behavior Therapy (DBT), facilitate healing and personal growth?
- What lessons can society learn from Stoicism in fostering compassion and understanding toward individuals with these disorders?
In an era increasingly aware of mental health issues, re-examining ancient wisdom offers valuable insights. By integrating philosophical and psychological perspectives, this analysis aims to provide a comprehensive understanding of the moral dimensions of NPD and BPD. It seeks to advocate for approaches that not only address clinical symptoms but also promote moral development and responsibility, aligning with the Stoic vision of achieving virtue through rational thought and self-awareness and, ultimately, advocating for a more empathetic and morally grounded approach to treatment and personal development.
¹ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), 43 (IV.3).
² Epictetus, The Enchiridion, trans. Elizabeth Carter, in The Stoic Philosophy of Epictetus (New York: Thomas Nelson and Sons, 1910), 11 (Chapter V).
³ American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), 645–659.
⁴ Albert Ellis, Reason and Emotion in Psychotherapy (Secaucus, NJ: Citadel Press, 1962), 63–78.
⁵ Carl Elliott, A Philosophical Disease: Bioethics, Culture, and Identity (New York: Routledge, 1999), 65–88.
⁶ Otto F. Kernberg, Borderline Conditions and Pathological Narcissism (New York: Jason Aronson, 1975), 27–45.
Chapter 2: Understanding Stoicism
“Men are disturbed not by things, but by the views they take of them.”¹
Origins and Historical Context
Stoicism is an ancient Greek philosophy founded in Athens by Zeno of Citium around 300 BCE.² Emerging during a period of social and political turmoil, Stoicism offered a path to personal tranquility amidst chaos. It was part of the Hellenistic philosophical traditions, which sought practical guidance for achieving eudaimonia — a state of flourishing or well-being.³
The philosophy gained prominence through the works of later Stoics such as Seneca, a Roman statesman; Epictetus, a former slave turned teacher; and Marcus Aurelius, a Roman emperor.⁴ Their writings have profoundly influenced Western thought, emphasizing ethics, logic, and natural philosophy.
Core Principles of Stoicism
At its core, Stoicism teaches that the path to a good life lies in the cultivation of virtue and wisdom. The central principles include:
Living in Accordance with Nature: This entails understanding the natural order of the world and aligning one’s actions accordingly.⁵ The Stoics believed that reason is a fundamental aspect of human nature, and living rationally leads to harmony with the cosmos.
The Discipline of Assent: Epictetus introduced the concept of distinguishing between what is up to us and what is not.⁶ What is up to us includes our own thoughts, desires, and aversions; what is not up to us involves external factors, such as other people’s actions or chance events.
Cultivation of Virtue: The four cardinal virtues in Stoicism are wisdom, courage, justice, and temperance.⁷ Virtue is considered the highest good and is sufficient for happiness.
Emotional Resilience: The Stoics posited that emotions result from judgments; by holding correct, rational judgments, one can achieve emotional tranquility and eudaimonia.⁸
The Stoic View on Emotions and Reason
Stoics believe that negative emotions stem from erroneous judgments.⁹ They argue that it is not external events that cause distress but our interpretations of those events. By applying reason, individuals can correct their false beliefs and attain peace of mind.
For example, if someone insults us, it is not the insult itself that harms us but our perception of it as injurious. By reframing our interpretation, we can remain unaffected.¹⁰ This cognitive reframing is a precursor to modern therapeutic techniques in psychology.
The Discipline of Assent
Epictetus emphasizes the proper use of prohairesis — our faculty of choice or moral will — by categorizing life into two distinct domains:
- What is up to us: Our thoughts, judgments, desires, and aversions.
- What is not up to us: External events, other people’s actions, and outcomes beyond our control.¹¹
By concentrating on what is up to us and accepting what is not, we can significantly reduce unnecessary suffering and achieve greater inner peace. This discipline of assent involves giving or withholding consent to impressions, ensuring that our judgments align with reason and virtue.
Virtue Ethics in Stoicism
Stoicism is a form of virtue ethics, asserting that moral character is the foundation of ethical behavior.¹² Virtue is not merely about adhering to rules but about developing excellent character traits. The Stoics believe that:
- Wisdom (Sophia): The ability to discern what is truly valuable and to make sound judgments.
- Courage (Andreia): Moral and psychological strength to face challenges and act rightly.
- Justice (Dikaiosyne): Fairness and integrity in dealings with others, respecting the rights and dignity of all.
- Temperance (Sophrosyne): Self-control and moderation in all aspects of life, avoiding excesses.
Achieving Tranquility and Eudaimonia
A natural consequence of living virtuously and rationally is eudaimonia, often translated as flourishing or well-being. This state involves:
- Self-awareness: Continuously examining one’s thoughts, emotions, and actions to ensure they align with virtue.
- Mindfulness: Being present and fully engaged in the moment, attentive to one’s internal and external environment.
- Acceptance: Embracing fate (amor fati) and understanding that everything happens according to a universal reason (logos).¹³
By embodying these principles, Stoics believe one can attain inner peace regardless of external circumstances. This philosophical approach offers practical guidance for navigating life’s challenges with equanimity.
¹ Epictetus, The Enchiridion, trans. Elizabeth Carter, in The Stoic Philosophy of Epictetus (New York: Thomas Nelson and Sons, 1910), 11 (Chapter V).
² Diogenes Laertius, Lives of Eminent Philosophers, trans. R. D. Hicks (Cambridge, MA: Harvard University Press, 1925), VII.1.
³ Julia Annas, The Morality of Happiness (New York: Oxford University Press, 1993), 21–34.
⁴ A. A. Long, Hellenistic Philosophy: Stoics, Epicureans, Sceptics (Berkeley: University of California Press, 1986), 107–145.
⁵ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), 9 (II.1).
⁶ Epictetus, The Enchiridion, 1.
⁷ Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 1969), 140–145 (Letter 76).
⁸ Margaret R. Graver, Stoicism and Emotion (Chicago: University of Chicago Press, 2007), 53–72.
⁹ Cicero, Tusculan Disputations, trans. J. E. King (Cambridge, MA: Harvard University Press, 1927), III.28.
¹⁰ Epictetus, Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008), 47–50 (I.25).
¹¹ Epictetus, The Enchiridion, 1.
¹² Julia Annas, The Morality of Happiness, 51–79.
¹³ Marcus Aurelius, Meditations, 57 (IV.23).
Chapter 3: The Stoic Sage vs. the Anti-Sage
“A good character is the only guarantee of everlasting, carefree happiness.”¹
The Stoic Sage: The Ideal of Moral Perfection
In Stoic philosophy, the sage represents the epitome of human excellence — a person who has achieved perfect wisdom and lives in complete harmony with nature and reason.² This figure embodies moral virtue, intellectual clarity, and emotional equilibrium. The Stoic sage not only comprehends what is good but also consistently acts upon it, seamlessly integrating knowledge and practice. The sage is characterized by complete virtue, exhibiting wisdom, courage, justice, and temperance in all actions.³ Emotional mastery is also a defining feature, as the sage remains free from the turmoil of irrational passions and experiences emotions that are aligned with reason.⁴ Their decisions are based solely on rational assessment and virtuous principles.⁵ This rationality enables the sage to maintain an unshakable calm and serenity even amidst adversity.⁶ Unlike those who seek happiness in material wealth or social approval, the Stoic sage finds happiness in internal virtue, achieving self-sufficiency.⁷
The Stoic sage understands the discipline of assent, recognizing that while external events are beyond personal command, responses to them are up to us.⁸ By focusing on what is “up to us,” the sage attains a state of eudaimonia, or flourishing, characterized by contentment and resilience.
The Anti-Sage: The Inverse of Stoic Virtue
In contrast to the sage is the conceptual opposite — the Anti-Sage — who embodies the antithesis of Stoic ideals. While the sage is guided by reason and virtue, the Anti-Sage is governed by passion, impulsivity, and moral vice.⁹ This figure lacks wisdom and self-control, succumbing to emotional disturbances and irrational desires. Decisions are driven by unchecked emotions rather than reason.¹⁰ The absence of the cardinal virtues or moral principles leads to unethical behavior.¹¹ The Anti-Sage is also characterized by emotional turmoil, being prone to distress, anger, envy, and other negative emotions.¹² Unlike the Stoic sage, whose happiness is derived from internal virtue, the Anti-Sage relies on material wealth, social status, or others’ opinions for happiness.¹³ Ignorance of the distinction between what is up to us and what is not further exacerbates the Anti-Sage’s instability.¹⁴
The Anti-Sage fails to practice the discipline of assent, reacting impulsively to external events and allowing passions to dictate actions.¹⁵ This results in a life characterized by dissatisfaction and instability, in stark contrast to the sage’s harmonious existence.
Personality Disorders as Manifestations of the Anti-Sage
When examined through a Stoic lens, certain personality disorders — specifically Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD) — exhibit traits akin to the Anti-Sage. These disorders represent significant deviations from Stoic virtues, dominated by irrational thoughts and emotional instability.
Individuals with NPD display grandiosity, an exaggerated sense of self-importance and entitlement.¹⁶ There is also a pervasive craving for external validation.¹⁷ Their lack of empathy and manipulative tendencies reveal a profound dependence on external factors for self-esteem, opposing the Stoic ideal of self-sufficiency.¹⁸ Manipulative behaviors are often employed to achieve personal goals.¹⁹
Similarly, individuals with BPD exhibit emotional instability, with rapid mood swings and intense emotions.²⁰ Fear of abandonment leads to extreme reactions to perceived or real separation.²¹ Impulsivity is evident in reckless behaviors that show little regard for consequences.²² Unstable relationships are marked by alternating between idealization and devaluation of others.²³
Both NPD and BPD manifest irrational thought patterns, distorted beliefs about oneself and others.²⁴ These individuals experience overwhelming emotions that lead to impulsive actions.²⁵ Their focus on external sources of happiness, rather than internal virtue, aligns them with the Anti-Sage’s reliance on passion over reason.²⁶
Irrational Thoughts and Emotional Turmoil
Albert Ellis, the founder of Rational Emotive Behavior Therapy (REBT), identified irrational beliefs as the root of emotional distress.²⁷ His framework echoes Stoic philosophy, particularly the notion that distorted thinking leads to negative emotions. Common irrational beliefs include demanding that life must conform to one’s desires, exaggerating the impact of adverse events, having a low tolerance for discomfort, and engaging in harsh self-criticism.²⁸-²⁹-³⁰-³¹ Individuals with NPD and BPD often exhibit these irrational beliefs, which fuel their emotional instability and maladaptive behaviors.³²
Stoicism advocates for recognizing false judgments, aligning thoughts and actions with reason, and regulating emotions to achieve tranquility.³³-³⁴-³⁵ By addressing irrational thoughts, individuals can reduce emotional turmoil and move toward the sage’s equanimity.
Splitting: A Barrier to Stoic Wisdom
In Object Relations Theory, splitting is a defense mechanism where individuals perceive themselves and others in black-and-white terms — either all good or all bad.³⁶ This inability to integrate positive and negative attributes leads to instability in self-image and relationships.
In NPD, splitting manifests as idealization of oneself as superior and flawless while devaluing others to maintain self-esteem.³⁷-³⁸ There is also heightened vulnerability to criticism, leading to overreactions to perceived slights.³⁹ In BPD, individuals experience extreme emotional shifts, alternating between idealization and devaluation of others.⁴⁰ Fear of rejection and unstable self-image contribute to intense interpersonal conflict.⁴¹-⁴²
The Stoic sage, in contrast, accepts complexity and recognizes the multifaceted nature of people and situations.⁴³ They practice moderation, avoiding extreme judgments and reactions.⁴⁴ The sage also cultivates unity of self, achieving coherence between thoughts, emotions, and actions.⁴⁵ Splitting hinders the development of wisdom by preventing a balanced understanding of reality.
Moral Responsibility and the Path to Virtue
Stoicism emphasizes that moral responsibility arises from our capacity for reason and choice.⁴⁶ While personality disorders present challenges, individuals are not absolved of moral accountability. There is potential for moral improvement through self-examination, cultivation of virtue, and emotional regulation skills.⁴⁷-⁴⁸-⁴⁹ Therapeutic approaches like Dialectical Behavior Therapy (DBT) teach mindfulness, distress tolerance, and emotional regulation, aligning with Stoic practices.⁵⁰ Cognitive-behavioral techniques are also effective in challenging irrational beliefs and promoting rational thinking.⁵¹ These approaches offer pathways toward moral and psychological growth.
The Road to the Sage: A Path of Healing
Transformation from the Anti-Sage to the Stoic sage involves self-reflection and acceptance, where individuals acknowledge irrational thoughts and emotional patterns and embrace reality as it is.⁵²-⁵³ The cultivation of virtue is essential, requiring a commitment to ethical principles and the development of character strengths through consistent practice.⁵⁴-⁵⁵ Emotional mastery is also crucial, achieved by applying reason to regulate emotional responses and practicing mindfulness to maintain present-moment awareness.⁵⁶-⁵⁷ Therapeutic support, such as DBT, provides tools and strategies aligned with Stoic ideals, while supportive relationships offer encouragement and aid in progress.⁵⁸-⁵⁹
Conclusion: Cultivating Virtue for a Harmonious Life
The contrast between the Stoic sage and the Anti-Sage underscores the profound impact of our thoughts and moral choices on well-being. While personality disorders pose significant obstacles, Stoic philosophy offers a roadmap for healing and personal development. By identifying irrational beliefs, cultivating virtue, and striving for emotional mastery, individuals can move closer to the Stoic ideal, achieving greater harmony within themselves and with others.
This transformation extends beyond the individual, contributing to a more compassionate and rational society. Stoicism, with its timeless focus on character and virtue, provides valuable insights for anyone seeking inner peace and ethical living.
¹ Seneca, Moral Letters to Lucilius, trans. Richard M. Gummere (Cambridge, MA: Harvard University Press, 1917), Letter 27.
² Diogenes Laertius, Lives of Eminent Philosophers, trans. R. D. Hicks (Cambridge, MA: Harvard University Press, 1925), VII.117.
³ Ibid., VII.92.
⁴ Margaret R. Graver, Stoicism and Emotion (Chicago: University of Chicago Press, 2007), 45–67.
⁵ Epictetus, Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008), I.1.
⁶ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), 57 (IV.23).
⁷ Ibid., 43 (IV.3).
⁸ Epictetus, The Enchiridion, trans. Elizabeth Carter, in The Stoic Philosophy of Epictetus (New York: Thomas Nelson and Sons, 1910), 1.
⁹ Julia Annas, The Morality of Happiness (New York: Oxford University Press, 1993), 409–411.
¹⁰ Albert Ellis, Reason and Emotion in Psychotherapy (Secaucus, NJ: Citadel Press, 1962), 63–78.
¹¹ Cicero, De Finibus Bonorum et Malorum, trans. H. Rackham (Cambridge, MA: Harvard University Press, 1914), III.7.
¹² Otto F. Kernberg, Borderline Conditions and Pathological Narcissism (New York: Jason Aronson, 1975), 22–35.
¹³ American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), 669–670.
¹⁴ Epictetus, Discourses, I.1.
¹⁵ Ibid., I.2.
¹⁶ APA, DSM-5, 669.
¹⁷ Ibid.
¹⁸ Ibid.
¹⁹ Kernberg, Borderline Conditions and Pathological Narcissism, 229–245.
²⁰ APA, DSM-5, 663.
²¹ Ibid.
²² Ibid.
²³ John G. Gunderson, Borderline Personality Disorder: A Clinical Guide, 2nd ed. (Washington, DC: American Psychiatric Publishing, 2009), 45–60.
²⁴ Ellis, Reason and Emotion in Psychotherapy, 87–102.
²⁵ Linehan, Marsha M., Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), 59–80.
²⁶ Kernberg, Borderline Conditions and Pathological Narcissism, 37–48.
²⁷ Ellis, Reason and Emotion in Psychotherapy, 35–62.
²⁸ Ibid., 69.
²⁹ Ibid., 73.
³⁰ Ibid., 77.
³¹ Ibid., 81.
³² Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, 101–125.
³³ Epictetus, Discourses, II.18.
³⁴ Marcus Aurelius, Meditations, 85 (VI.16).
³⁵ Graver, Stoicism and Emotion, 98–112.
³⁶ Ronald Britton, Belief and Imagination: Explorations in Psychoanalysis (London: Routledge, 1998), 45–58.
³⁷ Kernberg, Borderline Conditions and Pathological Narcissism, 19–21.
³⁸ Ibid., 22.
³⁹ APA, DSM-5, 670.
⁴⁰ Gunderson, Borderline Personality Disorder, 75–85.
⁴¹ Ibid., 60–74.
⁴² Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, 42–58.
⁴³ Marcus Aurelius, Meditations, 105 (VII.54).
⁴⁴ Epictetus, The Enchiridion, 33.
⁴⁵ Pierre Hadot, The Inner Citadel: The Meditations of Marcus Aurelius, trans. Michael Chase (Cambridge, MA: Harvard University Press, 1998), 83–97.
⁴⁶ Cicero, De Officiis, trans. Walter Miller (Cambridge, MA: Harvard University Press, 1913), I.11.
⁴⁷ Seneca, Moral Letters to Lucilius, Letter 83.
⁴⁸ Epictetus, Discourses, III.2.
⁴⁹ Graver, Stoicism and Emotion, 113–129.
⁵⁰ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, 137–162.
⁵¹ Ellis, Reason and Emotion in Psychotherapy, 123–147.
⁵² Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, 195–218.
⁵³ Epictetus, Discourses, I.12.
⁵⁴ Seneca, On the Shortness of Life, trans. C. D. N. Costa (London: Penguin Classics, 2004), 19.
⁵⁵ Hadot, The Inner Citadel, 117–130.
⁵⁶ Graver, Stoicism and Emotion, 130–150.
⁵⁷ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, 63–80.
⁵⁸ Ibid., 237–265.
⁵⁹ Gunderson, Borderline Personality Disorder, 150–165.
Chapter 4: Narcissistic and Borderline Personality Disorders
“Men are disturbed not by things, but by the views they take of them.”¹
— Epictetus, Enchiridion
Personality disorders are enduring patterns of inner experience and behavior that deviate markedly from cultural expectations, are pervasive and inflexible, and lead to significant distress or impairment.² Among these, Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD) — classified within Cluster B personality disorders — are particularly notable for their dramatic, emotional, and erratic presentations.³ Individuals with these conditions often exhibit intense emotions, impulsive behaviors, and unstable relationships, leading to substantial personal and interpersonal difficulties.
Core Beliefs in Narcissistic and Borderline Personality Disorders
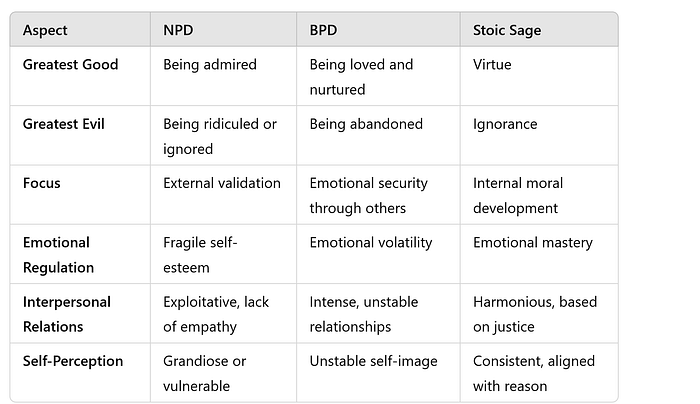
Psychologist Elinor Greenberg identifies distinct core beliefs that shape the worldviews of individuals with NPD and BPD, influencing their perceptions of the greatest goods and evils in life.⁴
Narcissistic Personality Disorder (NPD): At the core of NPD lies a preoccupation with admiration and a deep-seated fear of insignificance. For those with NPD, the greatest good is to be adored and respected, while the greatest evil is to be ridiculed, ignored, or diminished in the eyes of others.⁵ This distorted belief system drives behaviors aimed at securing admiration and avoiding criticism.
Individuals with NPD typically exhibit the following hallmark characteristics:
- Grandiosity: An exaggerated sense of self-importance and superiority.⁶
- Need for Admiration: A constant craving for external recognition and validation.⁷
- Lack of Empathy: Difficulty recognizing or caring about the feelings and needs of others.⁸
- Entitlement: An unreasonable expectation of especially favorable treatment or automatic compliance with one’s expectations.⁹
This intense need for admiration often leads individuals with NPD to manipulate others to maintain their inflated self-image. Their fragile self-esteem is heavily dependent on external approval, rendering them highly sensitive to criticism and prone to feelings of humiliation or emptiness when admiration is lacking.¹⁰
Borderline Personality Disorder (BPD): For individuals with BPD, the greatest good is being loved, cared for, and emotionally secure, while the greatest evil is abandonment or rejection, whether real or imagined.¹¹ This core belief results in pervasive anxiety about relationships and a relentless quest to avoid abandonment, even at the cost of personal well-being.
Key characteristics of BPD include:
- Fear of Abandonment: Intense anxiety over being left or rejected by significant others.¹²
- Unstable Relationships: Alternating between extremes of idealization and devaluation in relationships.¹³
- Identity Disturbance: A markedly unstable self-image or sense of self.¹⁴
- Emotional Instability: Rapid mood swings and intense emotional reactions.¹⁵
- Impulsivity: Engaging in potentially self-damaging behaviors without considering long-term consequences.¹⁶
The emotional volatility associated with BPD often leads to tumultuous relationships. The fear of abandonment may prompt impulsive actions such as clinging behaviors, emotional outbursts, or self-harm, which paradoxically can push others away, reinforcing the individual’s fears.¹⁷
The Stoic Sage: A Contrast in Values
The Stoic sage embodies an ideal of moral and emotional self-mastery. For the Stoic, the greatest good is virtue — the pursuit of wisdom, justice, courage, and temperance — and the greatest evil is ignorance, particularly of one’s own irrational thoughts and emotions that lead to unnecessary suffering.¹⁸ Unlike individuals struggling with personality disorders, the Stoic sage derives contentment and peace from within, through the cultivation of virtue rather than seeking approval or affection from others.
Comparative Analysis
While individuals with NPD and BPD are deeply tied to external factors — admiration for the narcissist and love and care for the borderline — the Stoic sage’s sense of self remains unshaken by external circumstances. This internal focus grants the sage emotional stability and resilience that those with personality disorders often lack.
The Pursuit of External vs. Internal Goods
The lives of individuals with NPD and BPD are marked by the pursuit of external goods that lie beyond their control:
- NPD: Happiness depends on admiration — a resource that must be continuously sought from others.
- BPD: Happiness lies in love and care — emotional security contingent on others’ willingness to provide it.
This dependence on external validation renders them vulnerable to emotional distress whenever their needs go unmet. Their self-worth is precarious, akin to a house built on sand.
In contrast, the Stoic sage seeks internal goods — virtues entirely within one’s control:
- Wisdom: Understanding what is truly good, bad, and indifferent.¹⁹
- Courage: Acting rightly despite fear or adversity.²⁰
- Justice: Treating others with fairness and integrity.²¹
- Temperance: Exercising self-control and moderation in all aspects of life.²²
By cultivating these internal virtues, the sage remains steady in the face of adversity, maintaining emotional balance regardless of external conditions.
Irrational Beliefs and Emotional Turmoil
Both NPD and BPD are fueled by deeply ingrained irrational beliefs:
- NPD: “I must be admired to be worthy.”
- BPD: “I cannot survive without being loved and cared for.”
These distorted beliefs align with what Albert Ellis described in Rational Emotive Behavior Therapy (REBT) as irrational demands — absolutist and unrealistic beliefs that lead to intense negative emotions and maladaptive behaviors.²³
Stoic Wisdom and Irrational Beliefs
Stoic philosophy teaches that such beliefs are illusions and sources of unnecessary suffering. According to Stoicism, it is not external events that disturb us but our judgments about them.²⁴ By identifying and challenging these irrational beliefs, individuals can free themselves from emotional turmoil and achieve peace of mind. The Stoic sage recognizes that true worth is found in virtue, not external validation.
The Impact on Behavior and Relationships
These irrational beliefs drive distinct patterns of behavior affecting both the individual and their relationships:
- NPD: The relentless pursuit of admiration can lead to manipulative behaviors, envy, and difficulty forming genuine, lasting relationships. Others may distance themselves due to the individual’s self-centeredness, leading to isolation.
- BPD: The intense fear of abandonment manifests in clinging behaviors, impulsivity, or self-sabotage. These actions strain relationships, often causing the very abandonment the individual fears.
The Stoic Sage: A Model for Healthy Relationships
In contrast, the Stoic sage, grounded in internal virtue, forms relationships based on mutual respect and justice rather than selfish desires. The sage is emotionally resilient, able to face loss or rejection without despair. This stability allows the sage to act with altruism, promoting the common good over personal gain.
Pathways to Transformation
Understanding the core values and irrational beliefs underlying NPD and BPD illuminates potential pathways for healing:
- Awareness: Recognizing the irrational beliefs that fuel distress.
- Reframing Values: Shifting focus from external validation to internal virtues.
- Self-Compassion: Building a sense of self-worth independent of others’ opinions.
- Mindfulness Practices: Cultivating present-moment awareness to reduce emotional reactivity.
Therapeutic approaches such as Dialectical Behavior Therapy (DBT) and Rational Emotive Behavior Therapy (REBT) offer tools for realigning beliefs and behaviors with Stoic principles.²⁵
Conclusion: Toward Emotional Resilience and Virtue
The contrast between the core values of individuals with NPD and BPD and those of the Stoic sage highlights the profound impact of beliefs on emotional well-being. By challenging irrational beliefs and cultivating internal virtues, individuals can move toward greater emotional resilience, stronger relationships, and a more stable sense of self.
In the journey from emotional volatility to tranquility, Stoic philosophy offers not only a path to personal peace but also a blueprint for living a life rooted in integrity and wisdom.
¹ Epictetus, The Handbook (Enchiridion), trans. Nicholas P. White (Indianapolis: Hackett Publishing Company, 1983), 5.
² American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), 645–684.
³ Ibid., 663–678.
⁴ Elinor Greenberg, Borderline, Narcissistic, and Schizoid Adaptations: The Pursuit of Love, Admiration, and Safety (New York: Greenbrooke Press, 2016), 25–47.
⁵ Ibid., 30.
⁶ American Psychiatric Association, DSM-5, 669.
⁷ Ibid.
⁸ Ibid.
⁹ Ibid.
¹⁰ Heinz Kohut, The Restoration of the Self (Chicago: University of Chicago Press, 1977), 105–110.
¹¹ Greenberg, Borderline, Narcissistic, and Schizoid Adaptations, 40.
¹² American Psychiatric Association, DSM-5, 663.
¹³ Ibid.
¹⁴ Ibid.
¹⁵ Ibid.
¹⁶ Ibid.
¹⁷ Marsha M. Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), 5–15.
¹⁸ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), 55.
¹⁹ Epictetus, Discourses, trans. Robert Dobbin (London: Penguin Books, 2008), 25–30.
²⁰ Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 2004), Letter 13.
²¹ Ibid., Letter 95.
²² Ibid., Letter 83.
²³ Albert Ellis, Reason and Emotion in Psychotherapy (New York: Lyle Stuart, 1962), 67–75.
²⁴ Epictetus, The Handbook (Enchiridion), 5.
²⁵ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder; Ellis, Reason and Emotion in Psychotherapy.
Chapter 5: Moral Responsibility and Personality Disorders
“A person with a personality disorder who behaves badly ordinarily intends to behave badly, and people should generally be held accountable for what they have intended to do.”
— Carl Elliott
The question of moral responsibility in the context of personality disorders such as Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD) presents a complex and nuanced challenge. While these disorders profoundly affect individuals’ thoughts, emotions, and behaviors, they often lead to actions that have significant moral and social implications, including manipulation, deceit, and harm to others. This chapter examines the debate over whether individuals with such disorders should be held morally accountable for their actions and explores the implications for treatment, legal considerations, and societal responses.
The Philosophical Debate on Moral Responsibility
Carl Elliott argues that personality disorders are fundamentally moral conditions as much as they are clinical ones.² He contends that individuals with personality disorders should be held responsible for their harmful actions because character flaws or psychological conditions do not absolve one of moral accountability. According to Elliott, a diagnosis of a personality disorder is not sufficient to excuse unethical behavior; rather, it highlights the need for moral reflection and responsibility.
Opponents of this view suggest that psychological disorders impair an individual’s judgment and ability to control their actions, thereby diminishing their culpability.³ They caution that labeling personality disorders as moral failings may increase stigma, hinder treatment, and overlook the complexity of these conditions. This perspective emphasizes the importance of compassion and understanding, recognizing that individuals with personality disorders often struggle with deep-seated emotional pain and distorted perceptions.
From a Stoic standpoint, there is an acknowledgment that while external factors and psychological conditions influence behavior, each person retains the capacity for reason and the potential to make virtuous choices.⁴ Stoicism teaches that individuals are responsible for their judgments and actions, and through the cultivation of wisdom and virtue, they can overcome irrational impulses and harmful behaviors.
Legal Implications and Therapeutic Jurisprudence
In legal contexts, the question arises as to whether individuals with personality disorders should be held criminally responsible for actions that violate societal norms and laws. Key considerations include whether the individual had the requisite intent (mens rea) and the ability to control their behavior at the time of the offense.⁵ Courts often grapple with the extent to which a personality disorder affects an individual’s capacity for self-control and moral reasoning.
Therapeutic jurisprudence offers an alternative approach, focusing on rehabilitation and the therapeutic potential of the legal system.⁶ Instead of emphasizing punishment, this perspective encourages accountability through restorative justice practices that aim to heal both the offender and the community. By addressing the underlying psychological issues and promoting moral development, therapeutic jurisprudence aligns with Stoic principles of personal responsibility and the pursuit of virtue.
The Role of Therapy in Moral Development
Dialectical Behavior Therapy (DBT), developed by Marsha M. Linehan, has proven effective in treating BPD by combining cognitive-behavioral techniques with mindfulness practices.⁷ DBT focuses on enhancing self-awareness, emotional regulation, distress tolerance, and interpersonal effectiveness. By helping individuals recognize and challenge irrational beliefs, DBT fosters the development of virtues such as honesty, empathy, and responsibility.
Similarly, therapies for NPD often incorporate elements of moral guidance, encouraging individuals to develop empathy and understand the impact of their actions on others.⁸ This process mirrors Stoic practices that emphasize self-examination, the cultivation of virtue, and adherence to moral principles.
Therapeutic interventions that integrate moral development address both the psychological and ethical dimensions of personality disorders. By promoting self-reflection and guiding individuals toward pro-social values, therapy can facilitate profound personal change and reduce harmful behaviors.
Challenges in Assigning Moral Responsibility
Personality disorders can distort perceptions and overwhelm rational thinking, making it difficult for individuals to make clear moral decisions. Symptoms such as impulsivity, emotional instability, and distorted self-image can impair judgment and self-control.⁹ Clinicians must navigate ethical considerations, balancing the need to hold individuals accountable with an understanding of their psychological limitations.
There is also the risk of imposing harsh judgments or moralizing in a way that may harm the therapeutic relationship.¹⁰ Therapists must respect the individual’s autonomy while guiding them toward greater self-awareness and moral responsibility. This requires a compassionate approach that acknowledges the challenges posed by the disorder while encouraging personal growth.
Societal Approaches: Balancing Accountability and Compassion
Society’s response to personality disorders should combine accountability with empathy. Education is crucial in reducing the stigma associated with NPD and BPD, fostering a more informed and compassionate understanding of these conditions.¹¹ By increasing public awareness, communities can encourage individuals to seek treatment without fear of judgment.
At the same time, it is essential to address harmful behaviors to protect the well-being of others. Legal and therapeutic systems can work together to provide opportunities for rehabilitation and personal development, rather than solely focusing on punishment. Restorative justice programs, for example, can facilitate healing by allowing individuals to make amends and engage in moral reflection.
The Potential for Moral Growth and Change
Despite the challenges posed by personality disorders, individuals with NPD and BPD retain the capacity for moral growth and transformation. Through therapy and self-examination, they can recognize irrational beliefs, develop virtues such as empathy and honesty, and embrace responsibility for their actions.¹² Success stories abound of individuals who have improved their relationships and overall well-being through integrated treatment approaches that combine psychological support with moral development.
This aligns with the Stoic view that individuals have the power to change their character through deliberate effort and the practice of virtue. Stoicism teaches that by focusing on what is within one’s control — namely, one’s own thoughts and actions — individuals can overcome destructive patterns and lead more fulfilling lives.¹³
Conclusion
Moral responsibility in the context of personality disorders requires a nuanced and compassionate approach that balances psychological understanding with ethical accountability. While NPD and BPD present significant challenges that can impair judgment and self-control, individuals are not devoid of moral agency. By combining therapeutic support with a focus on personal responsibility and virtue cultivation, individuals can transform their lives.
This integrated approach benefits not only the individuals themselves but also contributes to healthier communities and a more compassionate society. By fostering environments that encourage moral development and provide support, society can help individuals with personality disorders achieve meaningful change, reducing harmful behaviors and promoting overall well-being.
¹ Elliott, C., A Philosophical Disease: Bioethics, Culture, and Identity (New York: Routledge, 1999), p. 88.
² Ibid., pp. 85–89.
³ Morse, S. J., ‘Mental Disorder and Criminal Law’, Journal of Criminal Law and Criminology, 101.3 (2011), 885–968.
⁴ Epictetus, The Discourses, trans. R. Hard (London: Everyman’s Library, 1995), Book I, Chapter 1.
⁵ American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th edn (Arlington, VA: American Psychiatric Publishing, 2013), pp. 645–684.
⁶ Wexler, D. B., ‘Therapeutic Jurisprudence and Changing Conceptions of Legal Scholarship’, Behavioral Sciences & the Law, 11.1 (1993), 17–29.
⁷ Linehan, M. M., Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), pp. 19–28.
⁸ Ronningstam, E., ‘Narcissistic Personality Disorder: A Current Review’, Current Psychiatry Reports, 12.1 (2010), 68–75.
⁹ Kernberg, O. F., Borderline Conditions and Pathological Narcissism (New York: Jason Aronson, 1975), pp. 3–15.
¹⁰ Barnett, J. E., and Johnson, W. B., ‘Integrating Spirituality and Religion into Psychotherapy: Persistent Dilemmas, Ethical Issues, and a Proposed Decision-Making Process’, Ethics & Behavior, 21.2 (2011), 147–164.
¹¹ Hinshaw, S. P., and Stier, A., ‘Stigma as Related to Mental Disorders’, Annual Review of Clinical Psychology, 4 (2008), 367–393.
¹² Bateman, A., and Fonagy, P., Psychotherapy for Borderline Personality Disorder: Mentalization-Based Treatment (Oxford: Oxford University Press, 2004), pp. 50–70.
¹³ Marcus Aurelius, Meditations, trans. G. Hays (New York: Modern Library, 2002), Book II, Section 16.
Chapter 6: Irrational Thoughts and Negative Emotions
“If you are pained by any external thing, it is not this thing that disturbs you, but your own judgment about it.”¹
— Marcus Aurelius, Meditations
The Stoic philosophers posited that our emotional experiences are determined not by external events themselves but by the judgments and interpretations we ascribe to them. This insight is also fundamental in modern psychological therapies such as Cognitive Behavioral Therapy (CBT), Rational Emotive Behavior Therapy (REBT), and Dialectical Behavior Therapy (DBT). These approaches emphasize that irrational thoughts and beliefs are fundamental sources of negative emotions and maladaptive behaviors.
This chapter explores the intersection between Stoic philosophy and contemporary therapeutic practices, focusing on how both disciplines address irrational beliefs to promote emotional well-being and behavioral change. By examining how distorted thinking leads to emotional suffering, we highlight methods — both ancient and modern — for cultivating rational thought and emotional resilience.
Stoicism on Thoughts and Emotions
The Stoics believed that emotions result from judgments we make about external events, rather than the events themselves. They categorized emotions into two main groups: eupatheia (positive emotions) and pathē (negative passions). Positive emotions, such as joy and caution, arise when judgments align with reason and virtue. Negative passions, including anger, fear, and grief, stem from erroneous or irrational judgments about reality. By recognizing and correcting these false judgments, Stoics aimed to achieve apatheia — a state of inner tranquility and freedom from destructive emotions.²
A central concept in Stoicism is the role of “assent” (sunkatathesis), which refers to the moment when the mind agrees with or endorses an impression.³ Epictetus emphasized that external events are neutral and cannot disturb us on their own; it is our assent to these impressions that gives rise to emotional responses. He stated, “Men are disturbed not by things, but by the views they take of them.”⁴ By learning to withhold assent from misleading or irrational impressions, individuals can maintain equanimity in any situation.
Modern Psychological Therapies
Cognitive Behavioral Therapy (CBT): CBT is grounded in the principle that thoughts, feelings, and behaviors are interconnected.⁵ It teaches individuals to recognize and challenge distorted thinking patterns that contribute to emotional distress. Techniques such as cognitive restructuring involve identifying irrational or unhelpful thoughts and replacing them with more rational, adaptive ones. Behavioral activation encourages engagement in positive activities to improve mood and functioning.
Rational Emotive Behavior Therapy (REBT): Developed by Albert Ellis, REBT directly builds on Stoic principles by asserting that irrational beliefs are the root cause of emotional suffering.⁶ REBT focuses on identifying and disputing irrational beliefs — such as absolutist demands, overgeneralizations, and catastrophic thinking — and replacing them with rational, flexible alternatives that are more consistent with reality. This process involves examining the evidence for and against the irrational beliefs and considering more logical interpretations.
Dialectical Behavior Therapy (DBT): Initially designed by Marsha M. Linehan for treating Borderline Personality Disorder (BPD), DBT combines cognitive-behavioral techniques with mindfulness practices derived from Eastern contemplative traditions.⁷ DBT aims to help individuals manage intense emotions, reduce self-destructive behaviors, and improve relationships. It emphasizes four core skills: mindfulness, emotion regulation, distress tolerance, and interpersonal effectiveness.
Agreement Between Stoicism and Modern Therapies
Both Stoicism and modern psychological therapies share the understanding that our thoughts significantly influence our emotional states and behaviors. They assert that by changing maladaptive thought patterns, individuals can transform their emotional responses and improve their well-being. Additionally, both emphasize personal responsibility, encouraging individuals to actively engage in examining and adjusting their thinking processes.
In Stoicism, practices such as reflection, journaling, and premeditatio malorum — the anticipation of potential challenges — are used to cultivate emotional preparedness and rationality.⁸ Similarly, CBT employs techniques like thought records and cognitive reframing, where individuals document and analyze their thoughts to identify cognitive distortions and challenge them effectively.⁹
Common Irrational Thoughts and Their Reframing
One of the core teachings from both Stoicism and therapies like REBT is the importance of challenging irrational beliefs. For example, absolutist demands such as “Things must always go my way” or catastrophic thinking like “If something bad happens, it will be a disaster” can lead to unnecessary emotional turmoil. These beliefs can be reframed to promote a more rational and balanced perspective.
An irrational belief such as “I must always succeed, or I am worthless” can be restructured into a Stoic perspective: “While I prefer to succeed, my worth is not dependent on external outcomes.” Similarly, the thought “If someone criticizes me, it means they don’t value me” can be reframed as “Constructive criticism can be an opportunity for growth, and it does not define my value as a person.”
In the context of personality disorders, individuals with Narcissistic Personality Disorder (NPD) or Borderline Personality Disorder (BPD) often hold extreme, irrational beliefs. A person with NPD might believe, “I must be admired at all times, or I am nothing,” while someone with BPD may think, “If I am not constantly loved, I will be abandoned and cannot survive.” Through Stoic and therapeutic practices, these beliefs can be challenged and modified to promote healthier emotional regulation and a more stable sense of self.
Case Examples
Case of Narcissistic Personality Disorder: Consider an individual with NPD who becomes enraged when a colleague receives praise. The underlying irrational thought might be, “I deserve all recognition; if others are admired, it diminishes me.” Applying therapeutic techniques, this thought can be reframed to acknowledge that others’ successes do not detract from one’s own worth. The individual can adopt a Stoic perspective by recognizing that external validation is not the true measure of value and that focusing on personal virtue and integrity is more fulfilling.
Case of Borderline Personality Disorder: Imagine a person with BPD who panics when a friend does not immediately respond to a message. The irrational belief might be, “They are going to abandon me; I can’t handle being alone.” Therapy can help the individual consider alternative explanations for the delayed response and practice distress tolerance skills. From a Stoic viewpoint, the person can work on cultivating self-reliance and understanding that while relationships are important, their sense of worth and security should not be entirely dependent on others.
Strategies for Cultivating Rational Thinking
Stoicism and modern therapies offer various tools for promoting rational thinking and emotional resilience. Mindfulness practices, such as meditation and controlled breathing, help reduce rumination and enhance emotional clarity by keeping individuals grounded in the present moment.¹⁰ Socratic questioning — a method of systematically examining one’s beliefs — can uncover inconsistencies and cognitive distortions, allowing individuals to replace irrational thoughts with more logical alternatives.¹¹
Developing a philosophical outlook can also be a powerful means of cultivating resilience. Stoic exercises, such as reflecting on philosophical texts, engaging in daily self-examination, and aligning actions with core values, help individuals maintain a balanced perspective in the face of adversity. When combined with therapeutic strategies like cognitive reframing, these practices enable individuals to navigate life’s challenges with greater emotional stability.
The Role of Emotions in Personal Growth
Both Stoicism and modern therapies acknowledge that emotions are valuable signals that can provide insight into our internal states and external circumstances. However, they caution against allowing emotions to dominate reason. Rather than suppressing emotions, the goal is to understand and manage them effectively.
Emotional intelligence — the ability to recognize, understand, and regulate one’s emotions — is critical for personal growth.¹² It involves being aware of emotional triggers, understanding the beliefs and judgments that underlie emotional reactions, and employing strategies to manage these emotions constructively. By enhancing emotional intelligence, individuals can improve their relationships, decision-making, and overall well-being.
Conclusion
The convergence of Stoic philosophy and modern psychological therapies underscores the enduring importance of addressing irrational thoughts to overcome negative emotions and maladaptive behaviors. By cultivating rational thinking and emotional resilience, individuals can enhance their well-being and approach life’s inevitable challenges with greater calm and strength.
For those grappling with personality disorders like NPD and BPD, integrating Stoic principles with therapeutic techniques offers a viable path toward healing and personal development. It reaffirms the Stoic belief that while we may not control external events, we possess the power to shape our responses through the cultivation of reason and virtue. By embracing these practices, individuals can alleviate emotional suffering, foster a more stable sense of self, and move closer to living a life characterized by clarity, purpose, and inner peace.
¹ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), Book VIII, Section 47.
² Martha C. Nussbaum, The Therapy of Desire: Theory and Practice in Hellenistic Ethics (Princeton, NJ: Princeton University Press, 1994), pp. 359–360.
³ A. A. Long and D. N. Sedley, The Hellenistic Philosophers, Vol. 1 (Cambridge: Cambridge University Press, 1987), pp. 240–242.
⁴ Epictetus, The Handbook (Enchiridion), trans. Nicholas P. White (Indianapolis: Hackett Publishing Company, 1983), Section 5.
⁵ Judith S. Beck, Cognitive Behavior Therapy: Basics and Beyond, 2nd ed. (New York: Guilford Press, 2011), pp. 1–6.
⁶ Albert Ellis, Reason and Emotion in Psychotherapy, revised and updated edition (Secaucus, NJ: Citadel Press, 1994), pp. 27–35.
⁷ Marsha M. Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), pp. 19–28.
⁸ Donald Robertson, Stoicism and the Art of Happiness (London: Teach Yourself, 2013), pp. 85–90.
⁹ Beck, Cognitive Behavior Therapy, pp. 159–175.
¹⁰ Jon Kabat-Zinn, Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness (New York: Bantam Books, 1990), pp. 12–20.
¹¹ Aaron T. Beck, Cognitive Therapy and the Emotional Disorders (New York: Penguin Books, 1979), pp. 3–25.
¹² Daniel Goleman, Emotional Intelligence: Why It Can Matter More Than IQ (New York: Bantam Books, 1995), pp. 43–62.
Chapter 7: Splitting and Object Relations Theory
“Both you and I are citizens of the world; let us then adopt a citizen’s mindset and see the whole universe as our city.”
— Marcus Aurelius, Meditations
Object Relations Theory provides a psychoanalytic framework for understanding how early relationships shape an individual’s internal world and interpersonal dynamics. Central to this theory is the concept of splitting, a defense mechanism where a person perceives themselves and others in extremes — either all good or all bad.² This polarized thinking is particularly pronounced in individuals with Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD), where the inability to integrate complex emotional experiences leads to volatile relationships and unstable self-perceptions.³
This chapter delves into the nature of splitting within these disorders, examining how it disrupts the development of a cohesive self and balanced understanding of others. Drawing on Stoic philosophy, which emphasizes rational perception and emotional integration, we explore the psychological challenges of splitting and the therapeutic methods that promote healing and emotional wholeness.
Object Relations Theory
Object Relations Theory posits that early relationships, especially with primary caregivers, leave profound imprints that shape how individuals perceive themselves and relate to others throughout life.⁴ These early experiences form internal objects — mental representations of significant figures — that influence emotions and interactions. Ideally, as the psyche matures, these internal objects become more nuanced, allowing for the integration of both positive and negative aspects of self and others.⁵
Splitting, however, impedes this integration. Instead of reconciling contradictory feelings, individuals who engage in splitting oscillate between extremes: someone or something is either idealized or devalued, depending on the emotional context.⁶ This defense mechanism simplifies complex emotions to shield the individual from anxiety but sacrifices emotional and relational stability in the process.⁷
Splitting in Personality Disorders
Narcissistic Personality Disorder (NPD): In NPD, splitting manifests as grandiosity and vulnerability.⁸ The individual views themselves as superior and flawless, while others are dismissed if they fail to reinforce this inflated self-image.⁹ Criticism or perceived failure threatens their fragile sense of superiority, leading to overreactions, intense resentment, or complete devaluation of the critic.¹⁰ Relationships often become exploitative, with others reduced to instruments for maintaining self-esteem rather than partners in mutual respect.¹¹
Borderline Personality Disorder (BPD): In BPD, splitting contributes to emotional instability and fear of abandonment.¹² Individuals with BPD experience intense fluctuations in their perceptions of themselves and others, swinging from idealization to devaluation.¹³ Relationships are marked by rapid shifts: a person may be adored one moment and despised the next based on minor perceived slights.¹⁴ This instability stems from an unstable self-concept and a hypersensitivity to external feedback.¹⁵ The inability to integrate positive and negative aspects of experiences leads to volatile emotions and impulsive actions aimed at securing reassurance.¹⁶
The Stoic Perspective on Integration
Stoicism offers a counterbalance to the fragmented emotional world created by splitting. The Stoics believed that inner harmony and coherence are essential for a rational and fulfilled life.¹⁷ The self is guided by a rational soul that governs thoughts and actions.¹⁸ To achieve self-consistency, Stoicism encourages aligning beliefs, values, and behaviors, avoiding extremes that distort perception.¹⁹
Stoicism promotes the acceptance of complexity, recognizing that no person or situation is entirely good or bad.²⁰ By embracing imperfections in ourselves and others, we cultivate a balanced, universal perspective. The Stoic practice of reflecting on initial impressions before forming judgments helps prevent impulsive reactions driven by splitting.²¹ Instead of being swayed by volatile emotions, the Stoic aims for apatheia — a state of pleasant calm where reason governs responses to external events.²²
Therapeutic Approaches to Healing Splitting
Object Relations Therapy: Object Relations Therapy aims to help individuals integrate the fragmented parts of their psyche.²³ Therapists explore unconscious conflicts, particularly how early experiences with caregivers have shaped distorted internal objects. Through the therapeutic relationship, clients can rebuild trust and learn to perceive others more holistically, moving beyond oscillations between idealization and devaluation.²⁴
Dialectical Behavior Therapy (DBT): DBT has proven effective in treating BPD.²⁵ Combining cognitive-behavioral techniques with mindfulness, DBT addresses emotional dysregulation and black-and-white thinking associated with splitting.²⁶ By fostering present-moment awareness, DBT teaches individuals to observe their emotions without being controlled by them. The dialectical approach encourages acceptance of multiple, sometimes opposing truths, which is key to moving beyond all-or-nothing thinking.²⁷
Integrating Stoic Practices
Stoic practices offer practical tools for managing the emotional intensity of splitting. Cognitive distancing allows individuals to observe thoughts and emotions without immediate reaction, creating space for reasoned decision-making.²⁸ Stoicism emphasizes the cultivation of virtue — qualities like wisdom, courage, and temperance — that anchor the self in internal values or principles rather than external validation or fluctuating emotions.²⁹
Empathy is another crucial Stoic principle. By recognizing shared human experiences, individuals develop compassion for their struggles and the imperfections of others, softening rigid judgments caused by splitting.³⁰ This fosters healthier relationships and a more integrated sense of self.
Case Studies
Case of Narcissistic Personality Disorder: An individual with NPD feels humiliated by minor criticism at work. Initially, their self-image plummets, and they react by devaluing the person who offered the critique, labeling them as incompetent. Through therapy, the individual is encouraged to reflect on the intensity of their reaction and recognize that criticism, while uncomfortable, does not diminish their worth.³¹ A Stoic approach furthers this by helping the individual see that external opinions are indifferent to one’s internal virtue; true value lies in character, not constant admiration.³²
Case of Borderline Personality Disorder: A person with BPD feels devastated when a friend cancels plans, triggering intense feelings of abandonment. They may accuse the friend of being uncaring or reject them preemptively. Through DBT, they learn to pause, acknowledge their emotional surge without acting on it, and consider alternative explanations — perhaps the friend was simply unavailable.³³ A Stoic approach encourages acceptance of life’s uncertainties and focuses on cultivating self-sufficiency, recognizing that while relationships are valuable, one’s well-being should not solely depend on external sources.³⁴
The Journey Toward Full Object Relations
Healing from splitting involves developing a more integrated view of oneself and others. Accepting ambiguity — that people possess both positive and negative traits — is essential.³⁵ Strengthening the ego helps build a stable sense of self less reactive to external judgments.³⁶ Improved reality testing allows individuals to distinguish between emotional perceptions and objective facts.³⁷
Healthy relationships flourish when individuals maintain secure attachments built on trust, respect, and effective communication.³⁸ Setting and respecting boundaries is crucial for mutual understanding and personal well-being.³⁹ As individuals integrate their internal objects, they experience greater emotional stability and relational satisfaction.
Societal and Moral Implications
Splitting is not only an individual defense mechanism but also manifests at the societal level through polarized thinking.⁴⁰ Societies often divide groups or ideas into absolutes — good versus evil — leading to discrimination, conflict, and injustice.⁴¹ Overcoming these divisions requires cultural understanding, dialogue, and empathy — a collective effort to embrace complexity and recognize shared humanity.⁴²
Stoicism’s emphasis on universal citizenship and common reason offers a philosophical foundation for fostering social cohesion.⁴³ By promoting rational discourse and ethical behavior, societies can move beyond collective splitting toward more harmonious relations.⁴⁴
Conclusion
Splitting, while a protective mechanism against anxiety, ultimately hinders personal growth and the formation of healthy relationships. Understanding its roots within Object Relations Theory provides insight into the challenges faced by individuals with NPD and BPD. Therapeutic strategies like Object Relations Therapy and DBT offer effective means for addressing splitting and promoting emotional integration.
Stoic philosophy complements these therapeutic approaches by encouraging rational thinking, emotional balance, and acceptance of life’s complexities. By cultivating virtues and embracing a more nuanced perception of self and others, individuals can move toward greater emotional wholeness. Adopting the Stoic ideal that we are all citizens of the same human family underscores the interconnectedness of our struggles and aspirations, paving the way for collective healing and harmony.
¹ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), Book IV, Section 4.
² Melanie Klein, “Notes on Some Schizoid Mechanisms,” International Journal of Psycho-Analysis 27 (1946): 99–110.
³ Otto F. Kernberg, Borderline Conditions and Pathological Narcissism (Northvale, NJ: Jason Aronson, 1975), pp. 3–15.
⁴ Ronald Fairbairn, Psychoanalytic Studies of the Personality (London: Routledge, 1952), pp. 137–154.
⁵ W. R. D. Fairbairn, “The Repression and the Return of Bad Objects,” in An Object-Relations Theory of the Personality (New York: Basic Books, 1954), pp. 59–81.
⁶ Kernberg, Borderline Conditions and Pathological Narcissism, pp. 25–35.
⁷ Joan Symington, Narcissism: A New Theory (London: Karnac Books, 1993), pp. 45–50.
⁸ Elsa Ronningstam, “Narcissistic Personality Disorder: A Current Review,” Current Psychiatry Reports 12, no. 1 (2010): 68–75.
⁹ American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), pp. 669–672.
¹⁰ Kohut, Heinz, The Restoration of the Self (Chicago: University of Chicago Press, 1977), pp. 105–110.
¹¹ Campbell, W. Keith, and Joshua D. Miller, The Handbook of Narcissism and Narcissistic Personality Disorder (Hoboken, NJ: Wiley, 2011), pp. 201–215.
¹² Linehan, Marsha M., Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), pp. 5–15.
¹³ American Psychiatric Association, DSM-5, pp. 663–666.
¹⁴ John G. Gunderson, Borderline Personality Disorder: A Clinical Guide, 2nd ed. (Washington, DC: American Psychiatric Publishing, 2008), pp. 37–50.
¹⁵ Kernberg, Otto F., Severe Personality Disorders: Psychotherapeutic Strategies (New Haven, CT: Yale University Press, 1984), pp. 12–25.
¹⁶ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, pp. 35–40.
¹⁷ Epictetus, The Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008), Book II, Chapter 16.
¹⁸ Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 2004), Letter 41.
¹⁹ Long, A. A., Stoic Studies (Cambridge: Cambridge University Press, 1996), pp. 206–225.
²⁰ Epictetus, The Handbook (Enchiridion), trans. Nicholas P. White (Indianapolis: Hackett Publishing Company, 1983), Section 45.
²¹ Marcus Aurelius, Meditations, Book VIII, Section 7.
²² Brennan, Tad, The Stoic Life: Emotions, Duties, and Fate (Oxford: Oxford University Press, 2005), pp. 79–85.
²³ Greenberg, Jay R., and Stephen A. Mitchell, Object Relations in Psychoanalytic Theory (Cambridge, MA: Harvard University Press, 1983), pp. 10–25.
²⁴ Scharff, David E., and Jill Savege Scharff, Object Relations Individual Therapy (Northvale, NJ: Jason Aronson, 1998), pp. 75–90.
²⁵ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, pp. 19–28.
²⁶ Lynch, Thomas R., et al., “Dialectical Behavior Therapy for Borderline Personality Disorder,” Annual Review of Clinical Psychology 3 (2007): 181–205.
²⁷ Koerner, Kelly, Doing Dialectical Behavior Therapy: A Practical Guide (New York: Guilford Press, 2012), pp. 15–30.
²⁸ Robertson, Donald, Stoicism and the Art of Happiness (London: Teach Yourself, 2013), pp. 85–90.
²⁹ Irvine, William B., A Guide to the Good Life: The Ancient Art of Stoic Joy (New York: Oxford University Press, 2009), pp. 93–105.
³⁰ Seneca, On Clemency, trans. Susanna Braund (Chicago: University of Chicago Press, 2009), Book II.
³¹ Kohut, The Restoration of the Self, pp. 185–195.
³² Epictetus, The Discourses, Book I, Chapter 25.
³³ Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder, pp. 113–130.
³⁴ Epictetus, The Handbook (Enchiridion), Sections 8–10.
³⁵ Kernberg, Borderline Conditions and Pathological Narcissism, pp. 40–55.
³⁶ Fairbairn, Psychoanalytic Studies of the Personality, pp. 160–175.
³⁷ Gunderson, Borderline Personality Disorder: A Clinical Guide, pp. 70–85.
³⁸ Bowlby, John, Attachment and Loss, Vol. 1: Attachment (New York: Basic Books, 1982), pp. 345–355.
³⁹ Tatkin, Stan, Wired for Love (Oakland, CA: New Harbinger Publications, 2012), pp. 45–60.
⁴⁰ Klein, Notes on Some Schizoid Mechanisms, pp. 102–105.
⁴¹ Brewer, Marilynn B., “The Psychology of Prejudice: Ingroup Love or Outgroup Hate?” Journal of Social Issues 55, no. 3 (1999): 429–444.
⁴² Nussbaum, Martha C., Political Emotions: Why Love Matters for Justice (Cambridge, MA: Harvard University Press, 2013), pp. 360–375.
⁴³ Marcus Aurelius, Meditations, Book VI, Section 44.
⁴⁴ Sellars, John, Stoicism (Berkeley, CA: University of California Press, 2006), pp. 108–115.
Chapter 8: Comparative Analysis of Moral Values
“A good character is the only guarantee of everlasting, carefree happiness.”¹
— Seneca, Letters to Lucilius
Exploring moral values not only illuminates the foundations of individual behavior but also reveals the driving forces behind societal development. This chapter presents a comparative analysis of the moral values advocated by Stoic philosophy and those exhibited by individuals with Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD). By examining these contrasts and parallels, we gain insight into the essence of virtue, the roots of moral shortcomings, and possible pathways toward both personal and collective healing.
Core Moral Values: Stoicism vs. Personality Disorders
In Stoicism, virtue is the highest good. The Stoic sage embodies moral excellence through living in accordance with wisdom, courage, justice, and temperance.² Stoics assert that true happiness (eudaimonia) is derived from virtue alone, with external circumstances deemed indifferent.³ Ignorance, particularly of what is truly good or bad, leads to moral error and suffering.⁴ The Stoic goal is to cultivate a clear, rational view of the world, unclouded by false beliefs or emotional turmoil.
In contrast, individuals with NPD and BPD are guided by moral values centered on external validation and emotional security. Psychologist Elinor Greenberg identifies that for someone with NPD, the greatest good is being admired, while the greatest evil is being ridiculed or ignored.⁵ Their sense of self-worth is dependent on others’ approval. Similarly, individuals with BPD perceive the greatest good as being loved and cared for, and the greatest evil as abandonment.⁶ Their emotional well-being fluctuates with the stability of their relationships, rendering them vulnerable to extreme emotional reactions.
Where Stoicism seeks to ground happiness in internal virtues, the moral landscape of those with NPD and BPD is fragile, built on the shifting sands of external affirmation.
Integration vs. Splitting: Perceptions of Good and Evil
Stoicism teaches the acceptance of life’s inherent complexities. People, events, and circumstances are rarely purely good or purely bad; they are a mixture of both.⁷ Stoics cultivate a balanced view, guided by reason, that embraces this complexity. They emphasize the interconnectedness of humanity, recognizing that all individuals share both virtues and flaws.⁸ By accepting this, Stoics foster compassion, unity, and a rational understanding of the world.
In contrast, individuals with NPD and BPD often engage in a defense mechanism known as splitting, where they perceive themselves and others in extreme terms — either all good or all bad.⁹ This inability to reconcile contradictory feelings creates emotional chaos. They may idealize someone one moment and devalue them the next, struggling with the uncertainty that comes from seeing life in shades of gray.¹⁰ This all-or-nothing thinking destabilizes relationships and impairs moral development, as they find it difficult to navigate the ambiguity central to human experience.
The Role of Irrational Beliefs
At the heart of Stoicism is the alignment of beliefs with reality. Stoics stress the importance of challenging false judgments and understanding the world as it truly is, not as one wishes it to be.¹¹ They advocate living according to nature, accepting what cannot be changed, and maintaining emotional equanimity by focusing on what lies within one’s control.¹²
Individuals with NPD and BPD are often driven by irrational beliefs that distort their perceptions. For those with NPD, the belief that “I must always be admired, or I am worthless” creates an insatiable hunger for validation, leading to emotional dysregulation when they feel ignored or criticized.¹³ Similarly, individuals with BPD may hold the belief, “If I am not constantly loved, I will be abandoned and cannot survive.”¹⁴ This leads to intense emotional reactions and behaviors such as manipulation or self-harm, driven by the fear of rejection. These irrational beliefs fuel a cycle of emotional instability and moral conflict, as individuals may harm others to meet their own needs, or, paraphrasing Voltaire: “Those who believe absurdities commit atrocities.”
Moral Responsibility and Personal Transformation
Stoicism places great emphasis on personal responsibility in moral development. Self-examination is a critical practice, wherein individuals reflect on their thoughts, actions, and beliefs to cultivate virtue.¹⁵ Stoics believe that through actively practicing wisdom, courage, justice, and temperance, individuals can improve their character and lead lives aligned with moral principles. When mistakes occur, Stoics advocate taking responsibility, learning from errors, and continuing the pursuit of virtue.¹⁶
Modern therapies such as Cognitive Behavioral Therapy (CBT), Dialectical Behavior Therapy (DBT), and Rational Emotive Behavior Therapy (REBT) align with Stoic principles. These therapies emphasize challenging irrational beliefs, enhancing self-awareness, and developing healthier emotional and behavioral patterns.¹⁷ Through skill development in mindfulness, emotion regulation, and interpersonal effectiveness, individuals can cultivate empathy and compassion for themselves and others.¹⁸ These therapeutic approaches encourage individuals to take responsibility for their emotional states and actions, leading them toward greater self-understanding and moral growth.
Societal Implications: From Retribution to Restoration
On a societal level, splitting is not only an individual psychological defense but also manifests in how societies divide the world into simplistic dichotomies of good and evil.¹⁹ This tendency leads to cycles of retaliation and conflict, where opposing groups are dehumanized and treated as entirely bad. Historical patterns of retributive justice reflect this binary thinking, perpetuating cycles of violence and division.²⁰
Just as individuals can move beyond splitting through self-awareness and healing, societies can evolve toward more compassionate, nuanced moral frameworks. Shifting from retributive justice to restorative practices mirrors the evolution of morality from Lex Talionis (an eye for an eye), to the Stoic approach of understanding and integrating complexity.²¹ Restorative justice emphasizes healing and reconciliation over punishment, recognizing the shared humanity in all individuals.²²
The Journey Toward Integration and Virtue
For individuals with NPD and BPD, healing involves recognizing and challenging the irrational beliefs that govern their lives. By developing empathy, they begin to see others not as mere instruments of validation but as individuals with their own needs and emotions.²⁴ This growth leads to a more stable sense of self, where they can accept both their positive and negative qualities without resorting to extremes. Practicing virtues such as wisdom, justice, and temperance helps them build healthier, more fulfilling relationships.²⁵
Societies must undergo a similar process of integration. By rejecting simplistic dichotomies and embracing the complexity of human experience, communities can foster a more just and compassionate world.²⁶ Promoting restorative justice, encouraging moral growth, and creating inclusive spaces where differences are respected rather than feared allows for the healing of societal divisions.²⁷
Conclusion
This comparative analysis of moral values highlights the transformative potential for both individuals and societies. By moving away from splitting and irrational beliefs and embracing Stoic ideals of integration and virtue, healing becomes possible.
For individuals with NPD and BPD, the path forward involves questioning reliance on external validation, cultivating internal virtues, and building stronger, more empathetic relationships. For societies, the journey mirrors this personal transformation — rejecting simplistic divisions, fostering compassionate justice, and promoting moral growth.
Blending Stoic philosophy with modern therapeutic practices provides a powerful framework for addressing moral challenges facing individuals and communities. Recognizing our interconnectedness and striving toward virtue enables us to work toward a more harmonious and virtuous world.
¹ Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 2004), Letter 92.
² Epictetus, The Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008), Book I, Chapter 4.
³ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), Book II, Section 1.
⁴ Diogenes Laertius, Lives of Eminent Philosophers, trans. R. D. Hicks (Cambridge, MA: Harvard University Press, 1925), Book VII, Section 127.
⁵ Elinor Greenberg, Borderline, Narcissistic, and Schizoid Adaptations: The Pursuit of Love, Admiration, and Safety (New York: Greenbrooke Press, 2016), pp. 30–35.
⁶ Ibid., pp. 40–45.
⁷ Epictetus, The Handbook (Enchiridion), trans. Nicholas P. White (Indianapolis: Hackett Publishing Company, 1983), Section 1.
⁸ Marcus Aurelius, Meditations, Book VI, Section 44.
⁹ Melanie Klein, “Notes on Some Schizoid Mechanisms,” International Journal of Psycho-Analysis 27 (1946): 99–110.
¹⁰ Otto F. Kernberg, Borderline Conditions and Pathological Narcissism (Northvale, NJ: Jason Aronson, 1975), pp. 25–35.
¹¹ Epictetus, The Discourses, Book II, Chapter 18.
¹² Seneca, On the Shortness of Life, trans. C. D. N. Costa (London: Penguin Classics, 2004), pp. 1–10.
¹³ American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), pp. 669–672.
¹⁴ Ibid., pp. 663–666.
¹⁵ Seneca, Letters from a Stoic, Letter 16.
¹⁶ Marcus Aurelius, Meditations, Book V, Section 20.
¹⁷ Judith S. Beck, Cognitive Behavior Therapy: Basics and Beyond, 2nd ed. (New York: Guilford Press, 2011), pp. 1–6.
¹⁸ Marsha M. Linehan, Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), pp. 19–28.
¹⁹ Klein, “Notes on Some Schizoid Mechanisms,” pp. 102–105.
²⁰ Martha C. Nussbaum, Anger and Forgiveness: Resentment, Generosity, Justice (New York: Oxford University Press, 2016), pp. 15–30.
²¹ Howard Zehr, The Little Book of Restorative Justice (Intercourse, PA: Good Books, 2002), pp. 3–15.
²² Ibid., pp. 25–35.
²³ N. T. Wright, Evil and the Justice of God (Downers Grove, IL: InterVarsity Press, 2006), pp. 121–140.
²⁴ Bateman, Anthony, and Peter Fonagy, Psychotherapy for Borderline Personality Disorder: Mentalization-Based Treatment (Oxford: Oxford University Press, 2004), pp. 50–70.
²⁵ Epictetus, The Handbook (Enchiridion), Sections 33–38.
²⁶ Nussbaum, Anger and Forgiveness, pp. 218–230.
²⁷ Zehr, The Little Book of Restorative Justice, pp. 60–70.
Chapter 9: Therapeutic Approaches: From Moral Treatment to Healing
“The soul becomes dyed with the color of its thoughts.”¹
— Marcus Aurelius, Meditations
The convergence of moral development and psychological healing offers a unique pathway for addressing the complexities of Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD). These disorders, while clinically diagnosed, encompass moral dimensions that profoundly influence behavior and relationships. This chapter explores therapeutic approaches that integrate moral treatment with clinical interventions, aiming not only to alleviate symptoms but also to facilitate profound personal transformation and moral growth.
By examining therapies such as Dialectical Behavior Therapy (DBT), Cognitive Behavioral Therapy (CBT), and other integrative methods, we highlight how cultivating virtues aligned with Stoic philosophy can enhance treatment outcomes. The focus shifts from merely managing symptoms to fostering self-awareness, ethical living, and the development of healthier ways of relating to oneself and others.
Historical Context of Moral Treatment
In the 18th and 19th centuries, moral treatment emerged as a humane approach to mental health care. Pioneers like Philippe Pinel and William Tuke advocated for compassionate treatment of psychiatric patients, emphasizing respect, dignity, and personal responsibility.² Pinel removed the chains from patients at the Bicêtre Hospital in Paris, symbolizing a shift from confinement to care.³ Tuke established the York Retreat in England, where patients engaged in meaningful activities within a supportive community.⁴
These early practices recognized that treating patients with empathy and engaging them in purposeful pursuits could promote recovery. Moral treatment emphasized personal responsibility, social engagement, and ethical living, instilling values of honesty, cooperation, and self-discipline.⁵ However, the approach declined due to overcrowding in institutions and the rise of biological psychiatry in the late 19th century.⁶ In recent decades, its principles have resurfaced, integrated with modern psychological understanding to form more holistic therapeutic models.
Integrating Moral Development in Therapy
Virtue ethics, rooted in philosophical traditions like Stoicism, focuses on character development and the cultivation of moral virtues.⁷ In therapy, this translates to fostering self-reflection, moral reasoning, and character strengthening. Clients are encouraged to assess their values and behaviors, understand the ethical implications of their actions, and develop qualities such as honesty, empathy, and responsibility.
Integrating Stoic principles with therapy involves incorporating concepts such as the discipline of assent — helping clients distinguish between what is up to them and what is not.⁸ This empowers individuals to focus on their own judgments and choices rather than external circumstances. Emotional regulation techniques teach clients to manage passions and impulses, aligning with the Stoic aim of achieving inner tranquility.⁹ Mindfulness and presence cultivate awareness of thoughts and feelings without judgment, a practice central to both Stoicism and modern therapeutic approaches.
Dialectical Behavior Therapy (DBT)
Developed by Marsha M. Linehan for treating BPD, DBT combines cognitive-behavioral techniques with mindfulness practices derived from Eastern contemplative traditions.¹⁰ It addresses emotional dysregulation and interpersonal difficulties characteristic of BPD, aiming to help clients build a life worth living.
Core Components: DBT focuses on four primary skill areas: mindfulness, emotion regulation, distress tolerance, and interpersonal effectiveness.¹¹ Mindfulness enhances awareness of the present moment, teaching clients to observe and describe thoughts and feelings without immediate reaction. Emotion regulation involves understanding and managing intense emotions by identifying triggers, reducing vulnerability to emotional cues, and increasing positive experiences. Distress tolerance equips clients with strategies to withstand crises without resorting to harmful behaviors, employing techniques such as self-soothing and radical acceptance. Interpersonal effectiveness improves relationships through effective communication, assertiveness training, boundary setting, and balancing self-respect with relationship goals.
Moral Elements in DBT: DBT inherently incorporates moral development by emphasizing personal responsibility and commitment to change. Clients engage in a therapeutic contract, reflecting an active choice to pursue growth.¹² Validation and acceptance by therapists acknowledge clients’ feelings while guiding them toward healthier behaviors. The dialectical approach fosters flexibility, helping clients move beyond black-and-white thinking and embrace multiple perspectives.
Outcomes: Research indicates that DBT effectively reduces self-harm, suicidal behaviors, and hospitalizations among individuals with BPD.¹³ It enhances emotional regulation, strengthens relationships, and improves overall functioning. By integrating mindfulness and moral reasoning, DBT aligns with Stoic principles, promoting a balanced and virtuous life.
Cognitive Behavioral Therapy (CBT)
CBT is a structured, time-limited therapy that addresses dysfunctional thoughts and behaviors.¹⁴ Effective for various mental health conditions, including NPD and BPD, CBT is based on the premise that thoughts, feelings, and behaviors are interconnected.
Key Principles: CBT involves cognitive restructuring — identifying and challenging irrational beliefs — and behavioral activation, encouraging engagement in positive activities. Skills training develops coping mechanisms for stress and conflict. By addressing distorted thinking patterns, CBT fosters personal accountability, ethical decision-making, and empathy development.
Application to NPD and BPD: For NPD, CBT targets grandiose beliefs, entitlement, and lack of empathy. Clients learn to recognize and adjust distorted self-perceptions, enhancing interpersonal sensitivity.¹⁵ For BPD, CBT focuses on reducing impulsivity, stabilizing self-image, and improving emotional regulation.¹⁶ The therapy’s emphasis on challenging irrational thoughts parallels Stoic practices of examining and correcting false judgments.
Schema Therapy
Developed by Jeffrey Young, Schema Therapy integrates CBT with elements of attachment theory, object relations, gestalt therapy, and psychoanalytic concepts.¹⁷ It addresses deeply ingrained patterns of thought and behavior — schemas — that originate in childhood and persist into adulthood.
Focus on Maladaptive Schemas: Maladaptive schemas are enduring themes that influence self-perception and relationships.¹⁸ Schema Therapy aims to identify and modify these schemas, helping clients meet emotional needs in adaptive ways. The therapy combines cognitive techniques to challenge core beliefs, experiential techniques to process emotions, and behavioral strategies to develop new responses.
Relevance to Moral Development: By addressing unmet emotional needs and healing the “inner child,” Schema Therapy fosters compassion and empathy. Promoting the “Healthy Adult” mode encourages mature, responsible behavior aligned with moral values.¹⁹ This approach resonates with the Stoic focus on self-improvement and virtue cultivation.
Mentalization-Based Therapy (MBT)
MBT, developed by Peter Fonagy and Anthony Bateman, enhances the capacity to understand oneself and others in terms of mental states — thoughts, feelings, desires, and intentions.²⁰ Originally designed for BPD, MBT addresses deficits in mentalization that contribute to emotional dysregulation and interpersonal problems.
Key Concepts: MBT is grounded in attachment theory, recognizing that early relationships influence mentalization abilities.²¹ The therapy focuses on enhancing self-awareness, improving interpersonal understanding, and reducing reactive behaviors by fostering curiosity about mental states.
Moral Implications: By building empathy and promoting reflective functioning, MBT supports ethical relating and personal responsibility. Clients learn to consider the impact of their actions on others, aligning behavior with moral principles.²² This approach complements Stoic emphasis on self-examination and understanding the interconnectedness of human experiences.
Integrating Moral Philosophy into Therapy
Therapists can integrate Stoic practices such as daily reflection and journaling to encourage self-examination.²³ The premeditatio malorum — anticipating potential challenges — helps clients prepare emotionally for difficulties, fostering resilience.²⁴ Practicing virtues like wisdom, courage, justice, and temperance becomes a therapeutic goal, aligning actions with ethical values.
Engaging clients in discussions about personal values and moral dilemmas enhances moral reasoning.²⁵ Exploring hypothetical situations allows clients to consider the ethical implications of choices, while role-playing ethical responses reinforces practical application.
Therapists model virtues by demonstrating integrity, empathy, and respect.²⁶ Providing constructive feedback promotes growth, while creating a safe, non-judgmental environment facilitates open dialogue about moral concerns. The therapeutic relationship becomes a space for cultivating virtue and ethical awareness.
Case Studies
Individual Transformation: Healing NPD through Integrated Therapy
Background: John, a 35-year-old executive with NPD, exhibits grandiosity, lacks empathy, and struggles with relationships.
Therapeutic Approach: Combining CBT and Schema Therapy, John works on challenging beliefs about entitlement and superiority.²⁷ He addresses underlying schemas of defectiveness and vulnerability, engaging in exercises to develop empathy and moral reasoning.
Outcome: John increases self-awareness, recognizes patterns of manipulation, and begins to consider others’ feelings. Behavioral changes include improved interactions with colleagues and family, reflecting growth in moral character.
Individual Transformation: BPD Recovery through DBT and Stoicism
Background: Sarah, a 28-year-old teacher with BPD, experiences intense emotions, fear of abandonment, and self-harm behaviors.
Therapeutic Approach: Through DBT, Sarah learns emotion regulation and distress tolerance skills.²⁸ Incorporating Stoic practices, she engages in mindfulness and reflects on the dichotomy of control.
Outcome: Sarah stabilizes her emotions, reduces impulsivity, and establishes healthier boundaries. Developing a stronger sense of self, she moves toward self-acceptance and moral growth.
Challenges and Considerations
Clients may exhibit denial, fear of vulnerability, or reluctance to confront painful emotions.²⁹ Building a strong therapeutic alliance is essential to navigate resistance and encourage engagement.
Therapists must balance guidance with respect for client autonomy, avoiding imposing values while fostering moral development.³⁰ Cultural sensitivity is crucial, considering diverse backgrounds and belief systems.
Customization of therapy to individual needs requires flexibility and collaboration among professionals. Ongoing evaluation ensures effectiveness and allows for adjustments in strategies.³¹
The Societal Impact of Moral Healing
Personal healing extends to family dynamics, workplace culture, and community well-being.³² Improved relationships contribute to healthier environments, while ethical behavior enhances organizational integrity.
Reducing stigma involves promoting understanding of personality disorders and advocating for mental health initiatives that integrate moral considerations.³³ Encouraging empathy in schools and communities fosters social cohesion.
Conclusion
Therapeutic approaches that blend moral treatment with clinical interventions offer a holistic pathway to healing for individuals with NPD and BPD. By addressing both psychological and ethical dimensions, therapy facilitates profound personal transformation.
Emphasizing virtues aligned with Stoic philosophy — such as wisdom, courage, justice, and temperance — enables individuals to develop a strong moral compass. Integrating techniques from DBT, CBT, and other modalities enhances self-awareness, emotional regulation, and interpersonal effectiveness.
The journey from moral treatment to healing is not merely about symptom reduction but about fostering a richer, more meaningful life. It involves personal responsibility, empathy, and continuous moral growth. As individuals heal and grow, they contribute positively to society, embodying the Stoic ideal that personal virtue leads to collective well-being.
¹ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), Book III, Section 4.
² Bynum, W. F., The History of Medicine: A Very Short Introduction (Oxford: Oxford University Press, 2008), pp. 60–65.
³ Pinel, P., Traité médico-philosophique sur l’aliénation mentale (Paris: Richard, Caille & Ravier, 1801).
⁴ Digby, A., The Evolution of British General Practice 1850–1948 (Oxford: Oxford University Press, 1999), pp. 45–50.
⁵ Scull, A., Madhouse: A Tragic Tale of Megalomania and Modern Medicine (New Haven, CT: Yale University Press, 2007), pp. 25–35.
⁶ Shorter, E., A History of Psychiatry (New York: John Wiley & Sons, 1997), pp. 100–110.
⁷ MacIntyre, A., After Virtue (Notre Dame, IN: University of Notre Dame Press, 1981), pp. 181–203.
⁸ Epictetus, The Handbook (Enchiridion), trans. Nicholas P. White (Indianapolis: Hackett Publishing Company, 1983), Sections 1–5.
⁹ Irvine, W. B., A Guide to the Good Life: The Ancient Art of Stoic Joy (New York: Oxford University Press, 2009), pp. 93–105.
¹⁰ Linehan, M. M., Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993), pp. 19–28.
¹¹ Koerner, K., Doing Dialectical Behavior Therapy: A Practical Guide (New York: Guilford Press, 2012), pp. 15–30.
¹² Linehan, M. M., DBT Skills Training Manual, 2nd ed. (New York: Guilford Press, 2014), pp. 45–50.
¹³ Stoffers, J. M., et al., “Psychological Therapies for People with Borderline Personality Disorder,” Cochrane Database of Systematic Reviews 8 (2012): CD005652.
¹⁴ Beck, J. S., Cognitive Behavior Therapy: Basics and Beyond, 2nd ed. (New York: Guilford Press, 2011), pp. 1–6.
¹⁵ Ronningstam, E., “Narcissistic Personality Disorder: A Current Review,” Current Psychiatry Reports 12, no. 1 (2010): 68–75.
¹⁶ Arntz, A., “Cognitive Therapy versus Interpersonal Psychotherapy in the Treatment of Borderline Personality Disorder,” British Journal of Psychiatry 196, no. 5 (2010): 389–395.
¹⁷ Young, J. E., Klosko, J. S., and Weishaar, M. E., Schema Therapy: A Practitioner’s Guide (New York: Guilford Press, 2003), pp. 3–15.
¹⁸ Ibid., pp. 25–40.
¹⁹ Bernstein, D. P., Arntz, A., and de Vos, M., “Schema Focused Therapy in Forensic Settings: Theoretical Model and Recommendations for Best Clinical Practice,” International Journal of Forensic Mental Health 6, no. 2 (2007): 169–183.
²⁰ Bateman, A., and Fonagy, P., Mentalization-Based Treatment for Borderline Personality Disorder: A Practical Guide (Oxford: Oxford University Press, 2006), pp. 10–25.
²¹ Fonagy, P., Gergely, G., Jurist, E. L., and Target, M., Affect Regulation, Mentalization, and the Development of the Self (New York: Other Press, 2002), pp. 54–70.
²² Bateman, A., and Fonagy, P., “Randomized Controlled Trial of Outpatient Mentalization-Based Treatment versus Structured Clinical Management for Borderline Personality Disorder,” American Journal of Psychiatry 166, no. 12 (2009): 1355–1364.
²³ Robertson, D., Stoicism and the Art of Happiness (London: Teach Yourself, 2013), pp. 85–90.
²⁴ Pigliucci, M., How to Be a Stoic: Using Ancient Philosophy to Live a Modern Life (New York: Basic Books, 2017), pp. 120–130.
²⁵ Rest, J. R., Moral Development: Advances in Research and Theory (New York: Praeger, 1986), pp. 1–15.
²⁶ Beauchamp, T. L., and Childress, J. F., Principles of Biomedical Ethics, 7th ed. (New York: Oxford University Press, 2013), pp. 38–55.
²⁷ Beck, A. T., Freeman, A., and Davis, D. D., Cognitive Therapy of Personality Disorders, 2nd ed. (New York: Guilford Press, 2004), pp. 200–215.
²⁸ Linehan, M. M., DBT Skills Training Handouts and Worksheets, 2nd ed. (New York: Guilford Press, 2014), pp. 25–35.
²⁹ Prochaska, J. O., and Norcross, J. C., Systems of Psychotherapy: A Transtheoretical Analysis, 8th ed. (New York: Oxford University Press, 2018), pp. 275–290.
³⁰ Barnett, J. E., and Johnson, W. B., “Integrating Spirituality and Religion into Psychotherapy: Persistent Dilemmas, Ethical Issues, and a Proposed Decision-Making Process,” Ethics & Behavior 21, no. 2 (2011): 147–164.
³¹ Wampold, B. E., and Imel, Z. E., The Great Psychotherapy Debate: The Evidence for What Makes Psychotherapy Work, 2nd ed. (New York: Routledge, 2015), pp. 220–235.
³² Hinshaw, S. P., “The Stigmatization of Mental Illness in Children and Parents: Developmental Issues, Family Concerns, and Research Needs,” Journal of Child Psychology and Psychiatry 46, no. 7 (2005): 714–734.
³³ Corrigan, P. W., Druss, B. G., and Perlick, D. A., “The Impact of Mental Illness Stigma on Seeking and Participating in Mental Health Care,” Psychological Science in the Public Interest 15, no. 2 (2014): 37–70.
Chapter 10: Societal and Moral Implications
“Waste no more time arguing about what a good man should be. Be one.”¹
— Marcus Aurelius, Meditations
Understanding Narcissistic Personality Disorder (NPD) and Borderline Personality Disorder (BPD) as moral conditions, rather than solely clinical diagnoses, presents profound societal and moral implications. By embracing Stoic principles, we challenge conventional approaches to mental health, justice, and community well-being, advocating for a shift from punitive systems to restorative, compassionate practices. This chapter explores how integrating moral treatment can reshape societal attitudes and legal frameworks, promoting collective healing and fostering a more just and empathetic world.
Rethinking Mental Health and Moral Responsibility
Traditional mental health care often treats disorders like NPD and BPD as purely clinical issues, focusing on symptom management and behavioral modification.² However, acknowledging these disorders as moral conditions introduces the concepts of personal accountability and the potential for moral growth.³ Holistic treatment approaches that integrate moral reasoning and virtue development can lead to deeper transformation. This paradigm shift encourages empathy over stigma, suggesting that early education in emotional intelligence and ethical reasoning could help prevent the full development of personality disorders.⁴
From a Stoic perspective, individuals possess the capacity for rational thought and moral decision-making, regardless of their psychological challenges.⁵ By fostering self-awareness and emphasizing virtues such as wisdom, courage, justice, and temperance, therapy can help individuals with NPD and BPD cultivate a stronger moral compass.⁶ This approach aligns with modern therapeutic practices that focus on building emotional regulation and interpersonal skills, promoting both personal well-being and ethical behavior.
Legal and Ethical Considerations
Recognizing personality disorders as moral conditions raises complex questions of culpability within the legal system.⁷ Should psychological factors mitigate legal responsibility, or do individuals retain full accountability for their actions? Traditional punitive approaches may not address the underlying issues that contribute to criminal behavior among those with personality disorders.
Restorative justice offers an alternative by focusing on rehabilitation and healing rather than punishment.⁸ This model encourages offenders to take responsibility for their actions, make amends to victims, and reintegrate into society. Mental health courts, which specialize in cases involving psychological disorders, can provide tailored interventions that address both legal and therapeutic needs.⁹ By emphasizing accountability within a supportive framework, these courts facilitate personal growth and reduce recidivism.
This shift aligns with Stoic principles of justice and the belief that individuals can improve through self-reflection and ethical living.¹⁰ By addressing the root causes of harmful behavior, the legal system can contribute to societal well-being and the moral development of individuals.
Societal Attitudes and Stigma
Personality disorders are often misunderstood, leading to stigma and discrimination that create barriers to treatment.¹¹ Misconceptions perpetuated by media portrayals and lack of public education contribute to fear and marginalization of those affected.¹² This stigma can discourage individuals from seeking help and exacerbate feelings of isolation.
Public education campaigns and accurate media representations are vital for destigmatizing personality disorders.¹³ Advocacy groups and mental health professionals can promote awareness, emphasizing that NPD and BPD are treatable conditions with moral dimensions that can be addressed through therapy. By fostering empathy and understanding, society can encourage individuals to seek assistance without fear of judgment.
Moral Evolution of Society
Historically, societies have often favored retribution in response to wrongdoing, focusing on punishment rather than rehabilitation.¹⁴ Stoic philosophy suggests a shift toward compassion and understanding, recognizing that harmful behaviors often stem from irrational beliefs and emotional turmoil.¹⁵ By emphasizing rehabilitation and moral growth, society can cultivate forgiveness and support personal transformation.
Incorporating emotional and moral education into school curricula can help develop empathy, critical thinking, and ethical reasoning from an early age.¹⁶ These skills are essential for preventing the development of personality disorders and promoting a more compassionate society. Educational programs that teach emotional intelligence and conflict resolution contribute to healthier interpersonal relationships and community cohesion.
Building Resilient Communities
Communities play a crucial role in supporting mental health and fostering moral development. By creating environments that encourage social connection, provide resources, and promote inclusivity, communities can help mitigate the impact of personality disorders.¹⁷ Initiatives such as support groups, mentorship programs, and accessible mental health services strengthen social bonds and reflect the Stoic belief in interconnectedness.
Shared responsibility for one another’s well-being aligns with the Stoic concept of cosmopolitanism, which views all individuals as part of a global community.¹⁸ When communities invest in the mental and moral health of their members, they contribute to societal resilience and collective flourishing.
Ethical Leadership and Policy
Leaders have the power to influence societal values by promoting empathy, integrity, and justice. Policies that reflect compassionate approaches to mental health, combined with adequate funding for treatment programs, can lead to meaningful change.¹⁹ Public discourse that reduces stigma and encourages understanding is essential for progress.
Ethical leadership involves not only enacting policies but also modeling the virtues that promote moral development. By demonstrating commitment to the well-being of all citizens, leaders can inspire collective efforts toward a more just and empathetic society.
Cultural Narratives and Media Influence
Media shapes public perceptions of mental health, and harmful stereotypes contribute to misunderstanding and stigma.²⁰ Positive representations of recovery, resilience, and ethical behavior can inspire change. Public figures who speak openly about their experiences with mental health issues can reduce stigma and influence cultural narratives toward greater acceptance and empathy.²¹
Storytelling that humanizes individuals with personality disorders and highlights their potential for growth aligns with Stoic ideals of virtue and personal transformation. By shifting the narrative from one of fear and judgment to understanding and hope, media can play a pivotal role in societal healing.
Global Perspectives and Human Rights
Globally, mental health is recognized as a human rights issue. The World Health Organization (WHO) advocates for equitable access to mental health care and emphasizes its importance in overall human development.²² The United Nations (UN) highlights mental health within the context of human rights and sustainable development goals.²³
Ensuring dignity, respect, and cultural sensitivity in mental health care is a priority. International initiatives promote the integration of mental health services into primary care, community-based support, and the reduction of stigma worldwide.²⁴ These efforts reflect a global commitment to addressing the moral and societal implications of mental health disorders.
Case Studies: Societal Transformation
Community-based mental health programs provide tangible examples of how local support can reduce hospitalization rates and enhance social integration.²⁵ For instance, initiatives that involve peer support, family education, and community outreach have shown success in improving outcomes for individuals with personality disorders.
Restorative justice models applied to non-violent offenders with NPD or BPD have demonstrated success in reducing recidivism and facilitating rehabilitation.²⁶ Programs that focus on mediated dialogues between offenders and victims promote healing, accountability, and reintegration. These case studies highlight the benefits of shifting from punishment to healing, reflecting Stoic principles of justice and compassion.
The Role of Philosophy in Modern Society
Stoic principles, with their focus on reason, virtue, and emotional mastery, remain relevant in addressing contemporary societal challenges.²⁷ When integrated with other ethical traditions, such as Confucianism’s emphasis on harmony or Ubuntu’s focus on community, Stoicism promotes a global dialogue on moral growth.²⁸
This collective embrace of ethical values can lead to more compassionate policies and interactions at all levels of society. By encouraging individuals to cultivate inner virtues and contribute to the common good, philosophy serves as a guide for personal and societal transformation.
Challenges and Opportunities
Societal change faces resistance due to attachment to punitive models, resource limitations, and deep-seated stigmas.²⁹ Cultural barriers and misconceptions about mental health can hinder progress. However, technological advances, grassroots movements, and policy reform efforts offer opportunities to make lasting changes.
Digital platforms can facilitate education and support, expanding access to mental health resources.³⁰ Moments of political openness, or “policy windows,” can be leveraged to implement reforms.³¹ Empowering communities to lead change from the ground up ensures that initiatives are culturally relevant and sustainable.
Conclusion
Viewing NPD and BPD through the lens of moral conditions reshapes our approach to mental health and justice. By integrating Stoic philosophy, society can foster empathy, reform punitive systems, and enhance holistic treatment. This shift promotes personal responsibility, moral growth, and social well-being, reflecting a move toward the Stoic ideal of a rational, compassionate society.
Embracing these approaches aligns with the vision of a community where individuals contribute to the common good and support one another’s growth. As Marcus Aurelius advised, the time for debate is over; action is needed.³² Through collective efforts, we can create a world that not only addresses the challenges of personality disorders but also uplifts the human spirit.
¹ Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002), Book X, Section 16.
² American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013), pp. 645–684.
³ Elliott, C., A Philosophical Disease: Bioethics, Culture, and Identity (New York: Routledge, 1999), pp. 85–89.
⁴ Goleman, D., Emotional Intelligence: Why It Can Matter More Than IQ (New York: Bantam Books, 1995), pp. 285–300.
⁵ Epictetus, The Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008), Book I, Chapter 1.
⁶ Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 2004), Letters 16 and 71.
⁷ Morse, S. J., “Mental Disorder and Criminal Law,” Journal of Criminal Law and Criminology 101, no. 3 (2011): 885–968.
⁸ Zehr, H., The Little Book of Restorative Justice (Intercourse, PA: Good Books, 2002), pp. 3–15.
⁹ Wexler, D. B., “Therapeutic Jurisprudence and Changing Conceptions of Legal Scholarship,” Behavioral Sciences & the Law 11, no. 1 (1993): 17–29.
¹⁰ Long, A. A., Stoic Studies (Cambridge: Cambridge University Press, 1996), pp. 206–225.
¹¹ Hinshaw, S. P., and Stier, A., “Stigma as Related to Mental Disorders,” Annual Review of Clinical Psychology 4 (2008): 367–393.
¹² Pirkis, J., and Francis, C., “Mental Illness in the News and Information Media,” Australian Government Department of Health and Ageing (2007): pp. 1–50.
¹³ Corrigan, P. W., Druss, B. G., and Perlick, D. A., “The Impact of Mental Illness Stigma on Seeking and Participating in Mental Health Care,” Psychological Science in the Public Interest 15, no. 2 (2014): 37–70.
¹⁴ Nussbaum, M. C., Anger and Forgiveness: Resentment, Generosity, Justice (New York: Oxford University Press, 2016), pp. 15–30.
¹⁵ Marcus Aurelius, Meditations, Book IX, Section 42.
¹⁶ Payton, G., and Moody, L., “Emotional Intelligence in Education: A Critical Review,” Educational Research 48, no. 1 (2006): 127–142.
¹⁷ Putnam, R. D., Bowling Alone: The Collapse and Revival of American Community (New York: Simon & Schuster, 2000), pp. 402–414.
¹⁸ Sellars, J., Stoicism (Berkeley: University of California Press, 2006), pp. 108–115.
¹⁹ World Health Organization, Mental Health Action Plan 2013–2020 (Geneva: WHO Press, 2013), pp. 10–25.
²⁰ Stuart, H., “Media Portrayal of Mental Illness and Its Treatments,” CNS Drugs 20, no. 2 (2006): 99–106.
²¹ Wyllie, C., et al., Monitoring Change in Stigma: A Report to Time to Change (London: Institute of Psychiatry, King’s College London, 2012), pp. 5–20.
²² World Health Organization, Mental Health Atlas 2017 (Geneva: WHO Press, 2018), pp. 1–10.
²³ United Nations, Convention on the Rights of Persons with Disabilities (New York: United Nations, 2006), Articles 1–4.
²⁴ Patel, V., et al., “Addressing the Burden of Mental, Neurological, and Substance Use Disorders,” Lancet 374, no. 9690 (2009): 989–1003.
²⁵ Thornicroft, G., et al., “Community Mental Health Care Worldwide,” Harvard Review of Psychiatry 25, no. 5 (2017): 276–289.
²⁶ Braithwaite, J., Crime, Shame and Reintegration (Cambridge: Cambridge University Press, 1989), pp. 55–70.
²⁷ Robertson, D., Stoicism and the Art of Happiness (London: Teach Yourself, 2013), pp. 85–90.
²⁸ Wiredu, K., Cultural Universals and Particulars: An African Perspective (Bloomington: Indiana University Press, 1996), pp. 156–170.
²⁹ Walker, L. E. A., and Shapiro, D. L., “Resistance to Change: A Social Psychological Perspective,” in The Handbook of Organizational Culture and Climate, ed. N. M. Ashkanasy, C. P. M. Wilderom, and M. F. Peterson (Thousand Oaks, CA: Sage Publications, 2000), pp. 265–274.
³⁰ Naslund, J. A., et al., “The Future of Mental Health Care: Peer-to-Peer Support and Social Media,” Epidemiology and Psychiatric Sciences 25, no. 2 (2016): 113–122.
³¹ Kingdon, J. W., Agendas, Alternatives, and Public Policies, 2nd ed. (New York: Longman, 2003), pp. 165–195.
³² Marcus Aurelius, Meditations, Book XII, Section 1.
Further Reading
- American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013).
- Annas, Julia, The Morality of Happiness (New York: Oxford University Press, 1993).
- Aurelius, Marcus, Meditations, trans. Gregory Hays (New York: Modern Library, 2002).
- Cicero, Tusculan Disputations, trans. J. E. King (Cambridge, MA: Harvard University Press, 1927).
- Diogenes Laertius, Lives of Eminent Philosophers, trans. R. D. Hicks (Cambridge, MA: Harvard University Press, 1925).
- Ellis, Albert, Reason and Emotion in Psychotherapy (Secaucus, NJ: Citadel Press, 1962).
- Epictetus, Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008).
- Epictetus, The Enchiridion, trans. Elizabeth Carter, in The Stoic Philosophy of Epictetus (New York: Thomas Nelson and Sons, 1910).
- Elliott, Carl, A Philosophical Disease: Bioethics, Culture, and Identity (New York: Routledge, 1999).
- Graver, Margaret R., Stoicism and Emotion (Chicago: University of Chicago Press, 2007).
- Kernberg, Otto F., Borderline Conditions and Pathological Narcissism (New York: Jason Aronson, 1975).
- Long, A. A., Hellenistic Philosophy: Stoics, Epicureans, Sceptics (Berkeley: University of California Press, 1986).
- Seneca, Letters from a Stoic, trans. Robin Campbell (London: Penguin Classics, 1969).
References
- American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Arlington, VA: American Psychiatric Publishing, 2013).
- Annas, Julia, The Morality of Happiness (New York: Oxford University Press, 1993).
- Britton, Ronald, Belief and Imagination: Explorations in Psychoanalysis (London: Routledge, 1998).
- Cicero, De Finibus Bonorum et Malorum, trans. H. Rackham (Cambridge, MA: Harvard University Press, 1914).
- Cicero, De Officiis, trans. Walter Miller (Cambridge, MA: Harvard University Press, 1913).
- Diogenes Laertius, Lives of Eminent Philosophers, trans. R. D. Hicks (Cambridge, MA: Harvard University Press, 1925).
- Ellis, Albert, Reason and Emotion in Psychotherapy (Secaucus, NJ: Citadel Press, 1962).
- Epictetus, Discourses, trans. Robert Dobbin (London: Penguin Classics, 2008).
- Epictetus, The Enchiridion, trans. Elizabeth Carter, in The Stoic Philosophy of Epictetus (New York: Thomas Nelson and Sons, 1910).
- Graver, Margaret R., Stoicism and Emotion (Chicago: University of Chicago Press, 2007).
- Gunderson, John G., Borderline Personality Disorder: A Clinical Guide, 2nd ed. (Washington, DC: American Psychiatric Publishing, 2009).
- Hadot, Pierre, The Inner Citadel: The Meditations of Marcus Aurelius, trans. Michael Chase (Cambridge, MA: Harvard University Press, 1998).
- Kernberg, Otto F., Borderline Conditions and Pathological Narcissism (New York: Jason Aronson, 1975).
- Linehan, Marsha M., Cognitive-Behavioral Treatment of Borderline Personality Disorder (New York: Guilford Press, 1993).
- Marcus Aurelius, Meditations, trans. Gregory Hays (New York: Modern Library, 2002).
- Seneca, Moral Letters to Lucilius, trans. Richard M. Gummere (Cambridge, MA: Harvard University Press, 1917).
- Seneca, On the Shortness of Life, trans. C. D. N. Costa (London: Penguin Classics, 2004).